|
The inside of our body doesn't look like an anatomy textbook. It's an interesting phenomenon and one that I had never thought about before. I learned anatomy in college and I did so using images that highlighted the various muscles, nerves, and organs in different colors so they were easy to distinguish and identify. I never considered that my real nerves aren't yellow, that they are actually just about the same color as the muscles and blood vessels that surround them and that a surgeon, who sees these body parts on a daily bases, might have a hard time telling them apart. But after watching an amazing TED talk by Quyen Nguyen, a surgeon and professor of surgery at UCSD, I realized that one of the most difficult parts of surgery is figuring out what you're seeing.
Ideally, the anatomy textbook image would match with 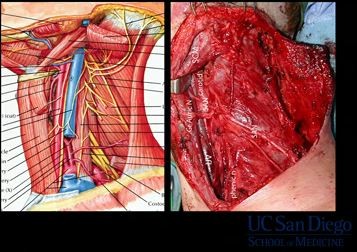 the real-life person. Nerves would be yellow, muscles brown, arteries red and veins blue. Then whatever wasn't supposed to be there, like a tumor or growth, would be some random color, easily identifiable and completely removable. Well, science is moving in that direction. Nguyen and her collaborator, Roger Tsien, are using fluorescents to color-code surgery. The team is using fluorescents to find and remove tumors more efficiently and effectively. Neck anatomy. Textbook vs. real life. Image Credit: UC San Diego. the real-life person. Nerves would be yellow, muscles brown, arteries red and veins blue. Then whatever wasn't supposed to be there, like a tumor or growth, would be some random color, easily identifiable and completely removable. Well, science is moving in that direction. Nguyen and her collaborator, Roger Tsien, are using fluorescents to color-code surgery. The team is using fluorescents to find and remove tumors more efficiently and effectively. Neck anatomy. Textbook vs. real life. Image Credit: UC San Diego.
The Problem
According to the American Cancer Society, there will be 1,638,910 new cancer cases in 2012. About 577,190 American's are expected to die of cancer this year, that's more than 1,500 people a day. Fortunately, research has led to us understanding things we can do in our day-to-day life to reduce our risk as well as treatments with very promising results. For patients who undergo surgery as part of their treatment, it can be a very frustrating process. If the entire tumor is removed with surgery, the patient is potentially cured of cancer, but how can surgeons remove all the cancer if they can't see it? The presence of tumor cells remaining in the surrounding area (the surgical margins) is called having positive margins and can cause the cancer to reoccur, resulting in additional radiation treatments and sometimes more surgery.
Currently, surgeons use guide wires to mark the outline of tumor. This technology relies on images seen on radiographic imaging or ultrasounds to distinguish tumors from healthy tissue. The difficulties come with the limited spatial resolution and in translating two-dimensional information to the three-dimensional surgical field. Another approach is to do immediate intraoperative (frozen) margin evaluation. The surgeon sends small samples from the tissues surrounding the surgical site to pathology where they freeze the sample and look for cancer cells with a microscope. This exchange happens several times until the results come back negative. The patient remains open and anesthetized in the OR while waiting for the results, increasing the chance of anesthesia-related complications and the length and cost of the surgery. It's also not a fool proof method and pathological results come back positive days after the patient has gone home.
The Discovery
The success of surgery aimed at removing a tumor (s) depends on the surgeon's ability to differentiate the tumor from normal tissue. The technique discussed in the TED talk comes out of research done at UC San Diego by Nguyen and her team which uses activatable cell-penetrating peptides (ACPPs). The fluorescently labeled polycationic cell-penetrating peptide (CPP) is coupled via a cleavable linker to a neutralizer. When the peptide is exposed to the proteases characteristic of the tumor cell, the linker is cleaved and the super sticky polycationic CPP binds to and enters the tumor cells, providing fluorescents.

Cell-penetrating peptides (CPPs) are composed of polycationic sequences of 6 to 12 consecutive arginines, which are covalently attached to a fluorophore called Cy5 ( a bright red pentamethine cyanine dye). The labeled CPPs are "sticky" meaning they can penetrate into most mammalian cells without specific receptors. By making them activatable CPPs (ACPPs), they are able to target the tumor. To prevent them from sticking to every cell they are linked to a neutralizing polyanionic peptide. The link is cleaved by a matrix metalloproteinases that are overexpressed in tumors. Image Credit: Dr. Roger Tsien
For the patient, this means that before their surgery they are injected with the ACPPs. The ACPPs travel to the tumor where the neutralizing link is cleaved. The ACPPs then stick to the tumor tissue. The surgeon shines a light on the area and the tumor glows, making it much easier for him or her to remove more of the tumor without leaving some behind. The surgeon can also use fluorescents to identify a nerve that finds the tumor to ensure they avoid causing nerve damage.
Future Possibilities
The practice of using fluorescents becoming a standard for surgeons doing surgery on cancer patients can have a dramatic effect on the quality of the patient's life. It could mean less time on the operating table and a reduction in the chance of reoccurrence or additional treatments for millions of people every year.
For more information watch the TED talk: Color-coded surgery.
Resources
Fluorescent Indocyanines for Color-Coded Surgery
Nguyen, Q. T., E. S. Olson, T. A. Aguilera, T. Jiang, M. Scadeng, L. G. Ellies, and R. Y. Tsien. "Surgery with Molecular Fluorescence Imaging Using Activatable Cell-penetrating Peptides Decreases Residual Cancer and Improves Survival." Proceedings of the National Academy of Sciences 107.9 (2010): 4317-322.
| 


 Re: Color-Coded Surgery: Lighting the Way for Surgeons
Re: Color-Coded Surgery: Lighting the Way for Surgeons